



The purpose of this article is to create a bridge between Orofacial Myofunctional Therapy (OMT) and the approach of the Postural Restoration Institute (PRI) with the ultimate goal of creating craniofacial resonance. To explain these ideas I am going to be discussing circles, aliens, a sticky orthotic, and some simple, silly, yet effective technique. I presented an earlier version of this blog post at the annual PRC/PRT Conference in Lincoln, Nebraska on April 22nd, 2017.
Before we get into the specifics of these relationships, I am going to go off on a bit of tangent. The purpose of which is to create a framework and context for which to hang OMT and PRI and how to integrate them into clinical practice.
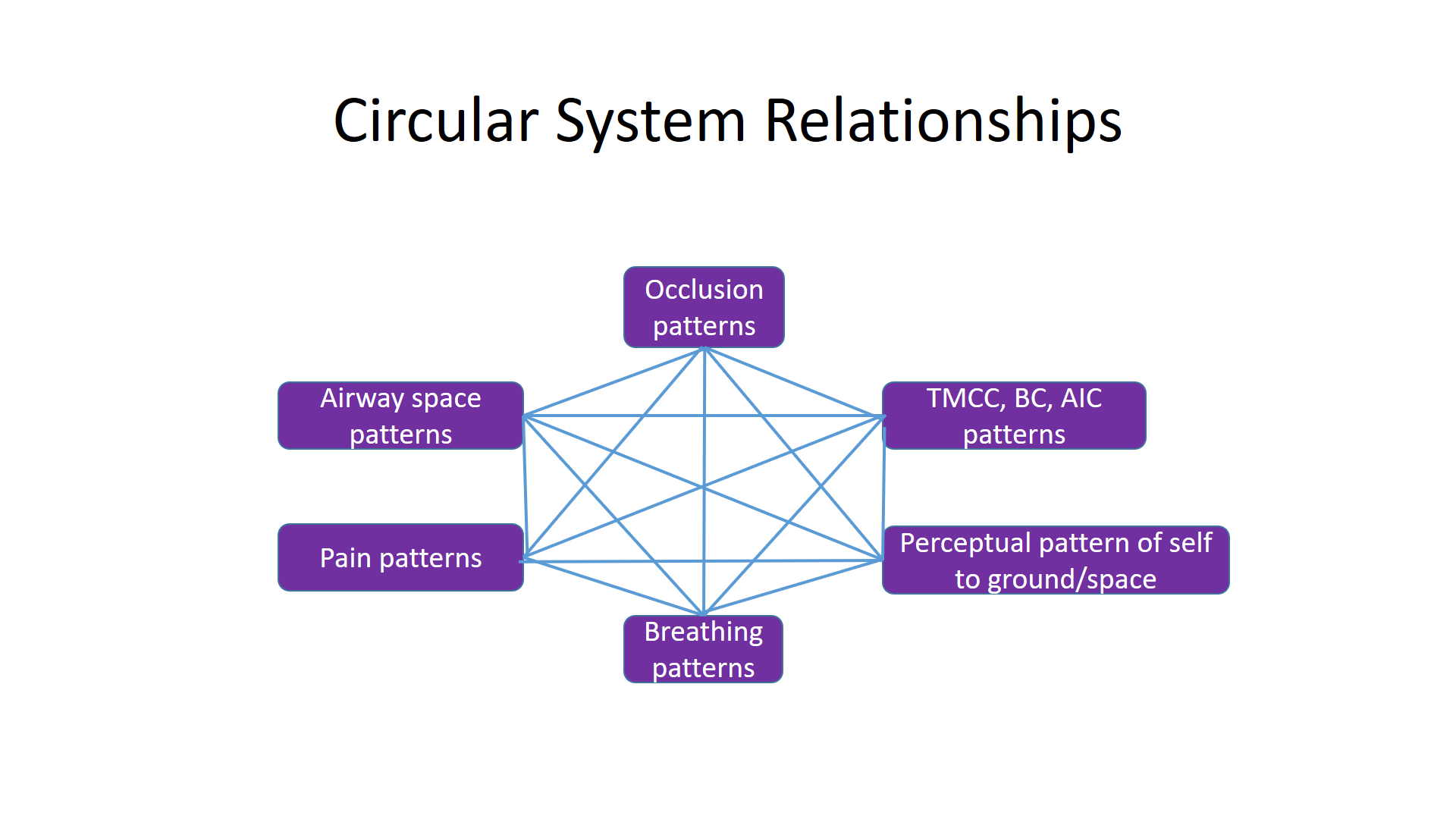
A couple months ago I was answering an email question regarding the connection between occlusion and neck pain. It was a challenging email to write out in a linear text fashion. There are so many factors involved in this relationship and they are all interrelated in terms of cause and effect. When I looked at my response I realized that I had explained my answer in an integrated circular manner.
This then got me thinking about the non-linear nature of time and reality and I thought about the movie “Arrival.” The premise of this film is that aliens, Heptapods to be more specific, unexpectedly visit our planet which puts humans in a tizzy because we are unsure of the true intention of their arrival. The main character, played by Amy Adams, is a linguist who has been assigned to learn how to communicate with the Heptapods and thus determine the true purpose of their visit. What she ultimately learns about their language is that their sentence structure is nonlinear because they ultimately perceive time as nonlinear in nature. Their reality is an interlacing circle of the past, present, and future perceived all at once.
I remember that as I watched this scene it occurred to me that this is how the mind of Ron Hruska (founder of PRI) operates and thus is a reflection of the PRI approach. For those who know Ron, he has a pattern of writing and speaking using complex sentences that take more time than usual to decode. For example, it took me 3 years to decode this particular sentence:
“Right occipital rotation on a left oriented atlas with left mandibular orientation, during left grounded stance reduces re-occurrence of right occipital rotation in left OA lateral flexion (L TMCC pattern) and right O on A and A on A rotation. “
(p. 38 2016 Cervical Revolution Manual/Postural Restoration Institute).
The purpose of putting this sentence up is not to discuss the specifics of these interrelated variables. That requires an understanding of multiple integrated three-dimensional spatial relationships of R vs L grounded stance patterns of the temporal cervical cranial mandibular system, which ones are pathological, and which ones are normal. There is an entire 2 day course that does this called Cervical Revolution. What I do want to do with this sentence is to look at it from the perspective of a Heptapod. This statement is ultimately depicting two different potential realities of L grounded stance, one with L occipital rotation and another with R occipital rotation based on the independent variable of L mandibular rotation.
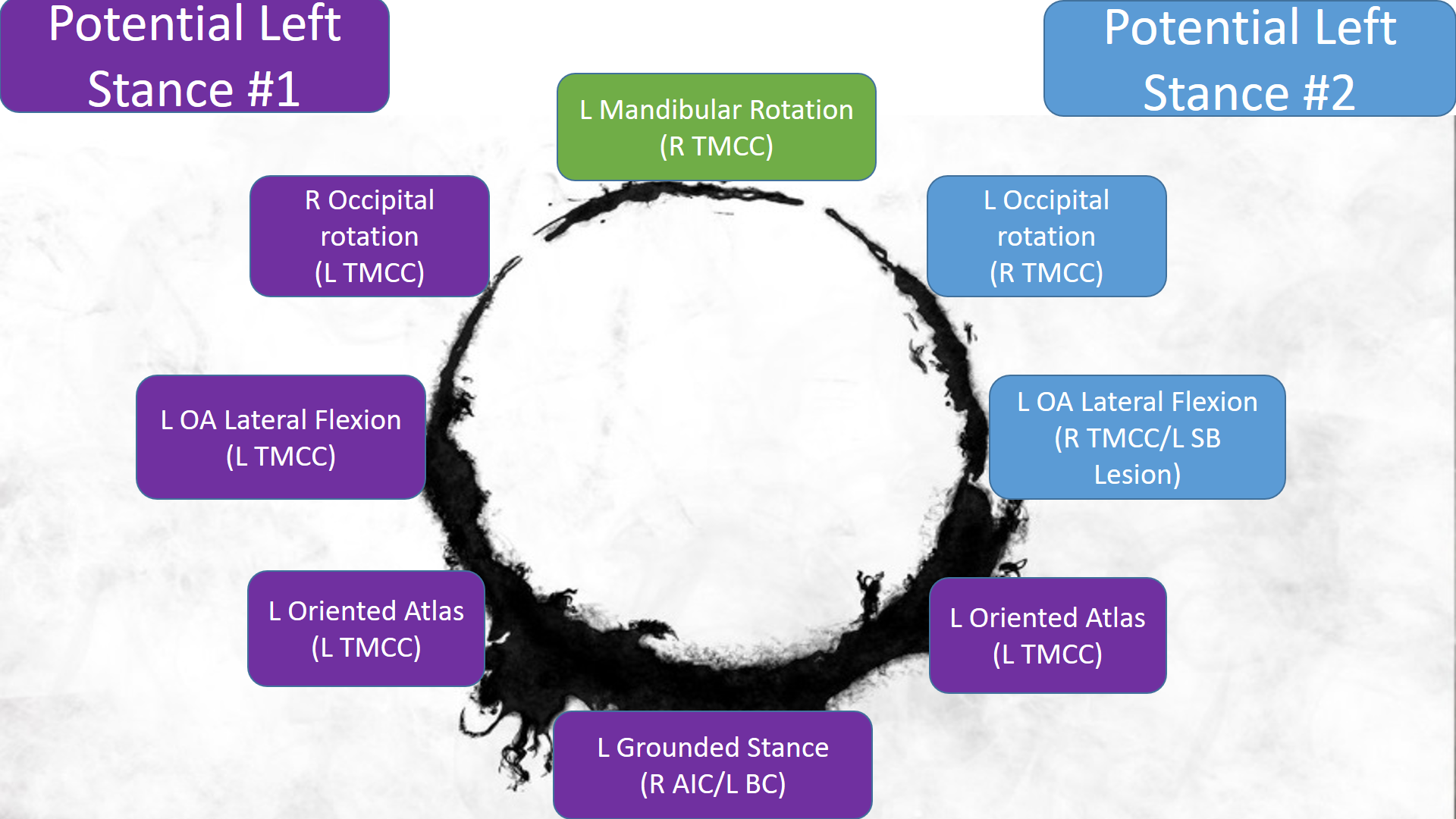
For those that have taken Cervical Revolution, isn’t this a bit easier to understand if written out this way?
After I saw Arrival I notified Ron that I had discovered his secret. I knew where he came from and who “his people” were. The truth is now out, Ron is a heptapod masquerading as a human. Just take a look at all these domed diaphragms and crura! I wonder where that obsession came from?

The reason I just used all this text and imagery to discuss the concept of circles is not only was it fun but because it is important to lay the context for which I am going to sew orofacial myofunctional therapy into a PRI perspective. It is but a sliver of the entire sphere where our intention is to ultimately create craniofacial resonance.
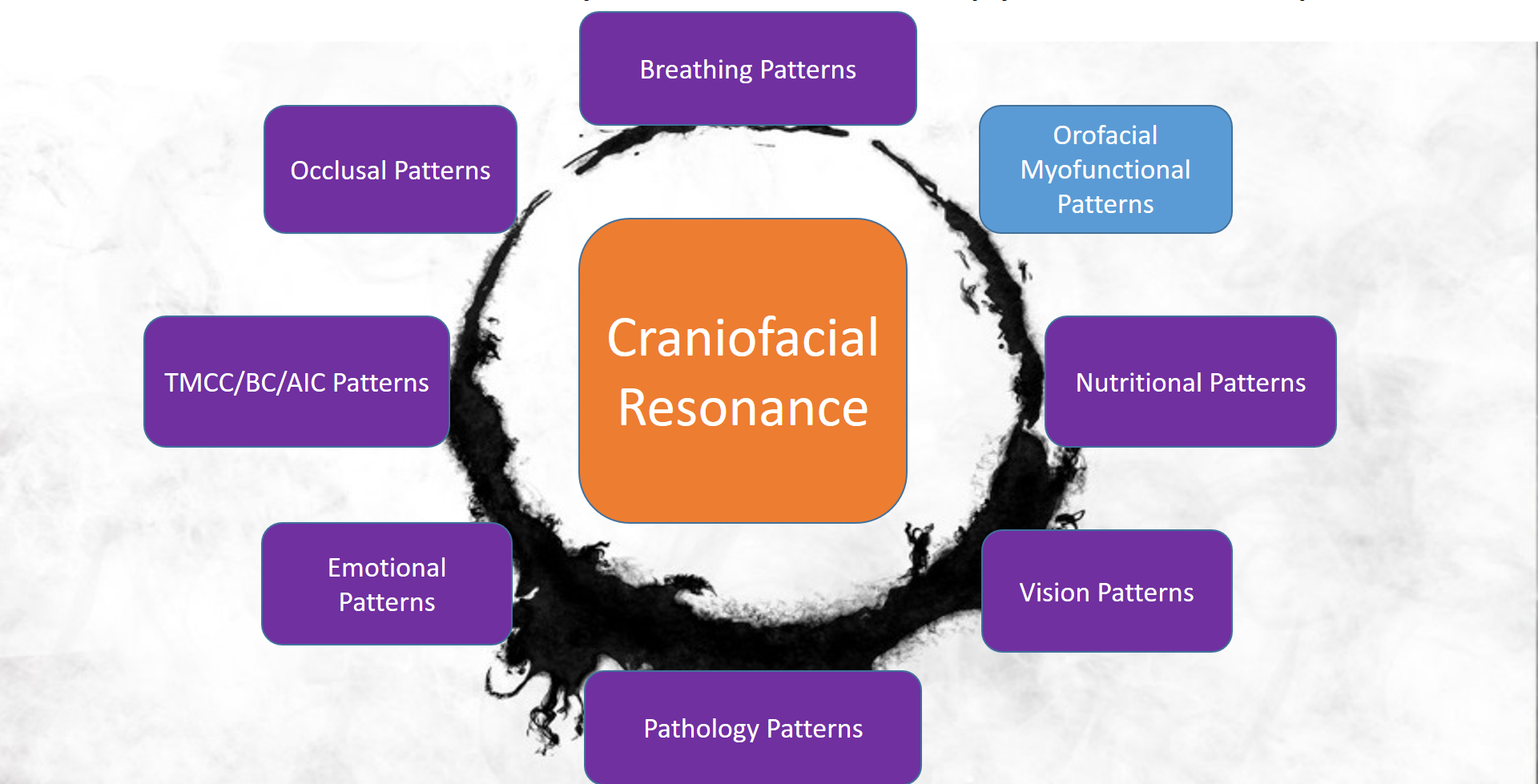
We typically refer to “reciprocal alternating motion” as the goal of PRI. This could also be regarded as resonance, a coherent vibration of shifting the body side to side. A resonating whole is predicated on the integration and sum of its resonating parts. The more systems you involve the more likely you can implement a change, create a new pattern, and thus resonate in tune. Our systems do not work in isolation but as an orchestrated symphony. As you can see above, OMT is but one component of the gestalt but personally and clinically it is perceived as a potentially potent one.
OMT may be defined as the neuromuscular re-education or repatterning of the oral and facial muscles to achieve proper tongue posture, breathing, chewing, and swallowing. In other words, it is about creating appropriate functional patterns of resonance via specifically training the orofacial system.
In the craniofacial world of PRI, the goal is to create alternating hemi-cranial extension and flexion patterns that correspond to the lateralized oscillations of gait. In PRI lingo this means authentic shifting of right and left TMCC (temporal mandibular cervical cranial chain) and thus resonance. This phenomenon is linked to the ability of one to achieve a “cranial zone of apposition” (ZOA), “facial hole control” (lip seal with nasal breathing), and a “upward and backward” swallow pattern. If any of these components are missing, it will be difficult to functionally resonate (chew, swallow, breathe, and also walk).
In “Connecting Postural Dysfunction, Craniofacial Development, and Nutritional Deficiencies”, the concept of a cranial ZOA is discussed in detail as well as potential causes of not having one. To briefly review these here, it is perceived that a cranial ZOA is the habitual posture of the tongue in full contact with the palate with the tip of the tongue against the alveolar ridge (not against the front teeth). This is analogous to the concept of a diaphragmatic ZOA where the thoracic diaphragm achieves a domed position in apposition (in contact) to the internal rib cage. We can take these comparisons another step further and relate how the pelvic floor diaphragm also maintains an elevated habitual position in states of functional balance.
The benefits of a cranial ZOA include:
- Facilitates forward and lateral development of the face during growth
- Maintains the shape of the dental arch
- Supports the head
- Promotes nasal breathing
- Enables proper speech production
- Serves as a brake to cranial torque driven by an asymmetrically powered diaphragm, visual system, and brain lateralization.
- Enables a swallow pattern that ultimately “pumps” the cranium facilitating CSF and lymphatic flow.
Potential interrelated factors that can limit a cranial ZOA are:
How does one assess a cranial ZOA? This is an integration point between PRI and OMT. Before you begin going down the cranial ZOA pathway you must first establish where your client/patient is with regards to their PRI tests. It is very important that they be aware of how they feel and what they see during their tests so that they have a reference point of comparison between pre and post-testing. For example, humeroglenoid internal rotation, abduction, and flexion can typically be both perceived and seen and thus easier to demonstrate a change. Cervical axial rotation, sidebending, and OA sidebending cannot typically be seen but felt. Straight leg raise is also a good test to use as cranial ZOA restoration typically influences this motion. Of course you may do any tests you choose and desire to make and demonstrate a change.
After you have established your PRI measurements and allowed your patient/client to sense where they are at, it is time to determine the habitual rest position of their tongue. Through this questioning, explain to your patient/client the different components of their palate. Anteriorly, this includes the alveolar ridge (above inner front incisors angling up and back until it meets the hard palate. From here, conceptually break up the hard palate into an anterior ½ and posterior ½. Posteriorly, there is the downward sloping soft palate. After explaining the concept of these “parts” have the patient/client determine where they habitually posture. The ideal position is to have complete contact against the entire hard palate, anterior soft palate, with the tip against the alveolar ridge. If they are already there then great! They have a cranial ZOA! If they aren’t then you need to determine the amount of contact they can achieve. How far back can they sense and make contact with their tongue with the tip of the tongue on the alveolar ridge?
If they are limited in posterior contact points the following manual technique (I refer to this as the cranial ZOA Restoration Technique) may be applied to achieve full tongue/palate apposition. This technique accomplishes both a fascial stretch as well as neuromuscular inhibition to the muscles that prevent the tongue from elevating. The Institute for Physical Art has a version of this technique which I learned about through fellow Physical Therapist, Brad Gilden.

Wrap a napkin or paper towel (something with relative thickness and texture) around the tongue, close to the anterior base of the tongue. You may feel a fibrous, central, tendonous, tissue here (frenulum). Grip around the tongue with the thumbs at the frenulum and gently pull the tongue up towards the hard and posterior soft palate (wherever the apposition is limited) until a stretch is felt. Direct the amount of force by opening and closing the jaw. One may also open and move the jaw side to side to get different fibers to stretch. Perform for 1-2 minutes and repeat frequently throughout the day. Laying supine is typically the easiest position to perform this but it can also be done in the sitting and standing positions. I typically perform this technique on my patient and then teach them for self-application.
After performing the technique, have the patient/client reassess how much contact they have. Usually, they should feel more apposition posteriorly. Once this is established then take them through their PRI tests to determine the extent that their cranial ZOA is having on the rest of the postural system. Now its time for the “wow” factor as they typically are blown away by how this can create such significant changes. If it does, then it is appropriate to proceed with further intervention to establish a consistent cranial ZOA. If it doesn’t, then its time to move on to another variable as this one has proven to not be significant for their system.
If after a few weeks of diligent performance of the manual and non-manual techniques (to be described later in this article) and there is no significant improvement, consideration of a frenectomy would be appropriate. If a frenectomy is going to be performed the success of this procedure is dependent on immediate performance of orofacial myofunctional therapy techniques afterwards (same day) to prevent scarring. A positive outcome is also facilitated by performing the techniques prior to the frenectomy so that the tongue can begin to develop some sensori-motor awareness and function that is often limited in cases involving tongue ties. To learn more about tongue ties you may reference “Connecting Postural Dysfunction, Craniofacial Development, and Nutritional Deficiencies.”
We are now in a position to begin training the tongue and orofacial complex for the goal of adopting a habitual cranial ZOA. Like acquiring any other new skill, this process requires a period of significant cognitive effort. The individual will have to consciously work at training this new behavioral pattern. One of the ways to do this is to place a small rubber band (such as those used in orthodontia) on the top of the tongue to serve as a sensory reminder to keep it in contact with the palate. This can be done in circumstances where the individual does not have to talk such as when working on a computer, driving, or watching TV. I give credit to Joy Moeller for teaching this to me. Joy is also credited with getting orofacial myofunctional therapy on the map, establishing the Academy of Orofacial Myofunctional Therapy, and taught me the majority of the techniques I am going to discuss through her 4 day course titled, “AOMT Comprehensive Introduction to Orofacial Myofunctional Therapy.” I encourage you to check out AOMT’s website (https://aomtinfo.org/) to learn more about OMT and opportunities for learning more about it.
In situations regarding a tongue tie, techniques that incorporate multi-directional movement of the tongue serve not only to promote flexibility but sensorimotor education as well. For individuals who have had restricted motion capability of their tongue all their life, they will now be able to move their tongue in ways they have NEVER experienced before. In a way, you are taking them back in time through the developmental processes that should have occurred in the womb and early life.
The “Monkey” and “Monkey Circles” help to accomplish continued tongue flexibility as well as provide a sensorimotor experience. Simply place your tongue between your front teeth and lips and either hold this for ~30 seconds and/or make circles (clockwise and counterclockwise) between the lips and front teeth. It’s amazing how tiring this can be for the tongue!
Side Note: Special thanks for my handsome husband, Jan, for agreeing to be my face model for the following, not always flattering, pictures:)

The “Snake” coupled with multi-directional tongue slides is another option. Point the tongue straight out, hold for ~ 5 sec, then slide the tongue posteriorly attempting to make contact with the posterior tongue on the soft palate. You can also do side to side (frontal plane) sweeps where the tongue moves between the outer teeth and cheeks, over the molars, the palate, over the molars on the other side, and between the outer teeth and cheeks. You can also “waggle” the “snake” and move the tongue side to side outside the mouth.
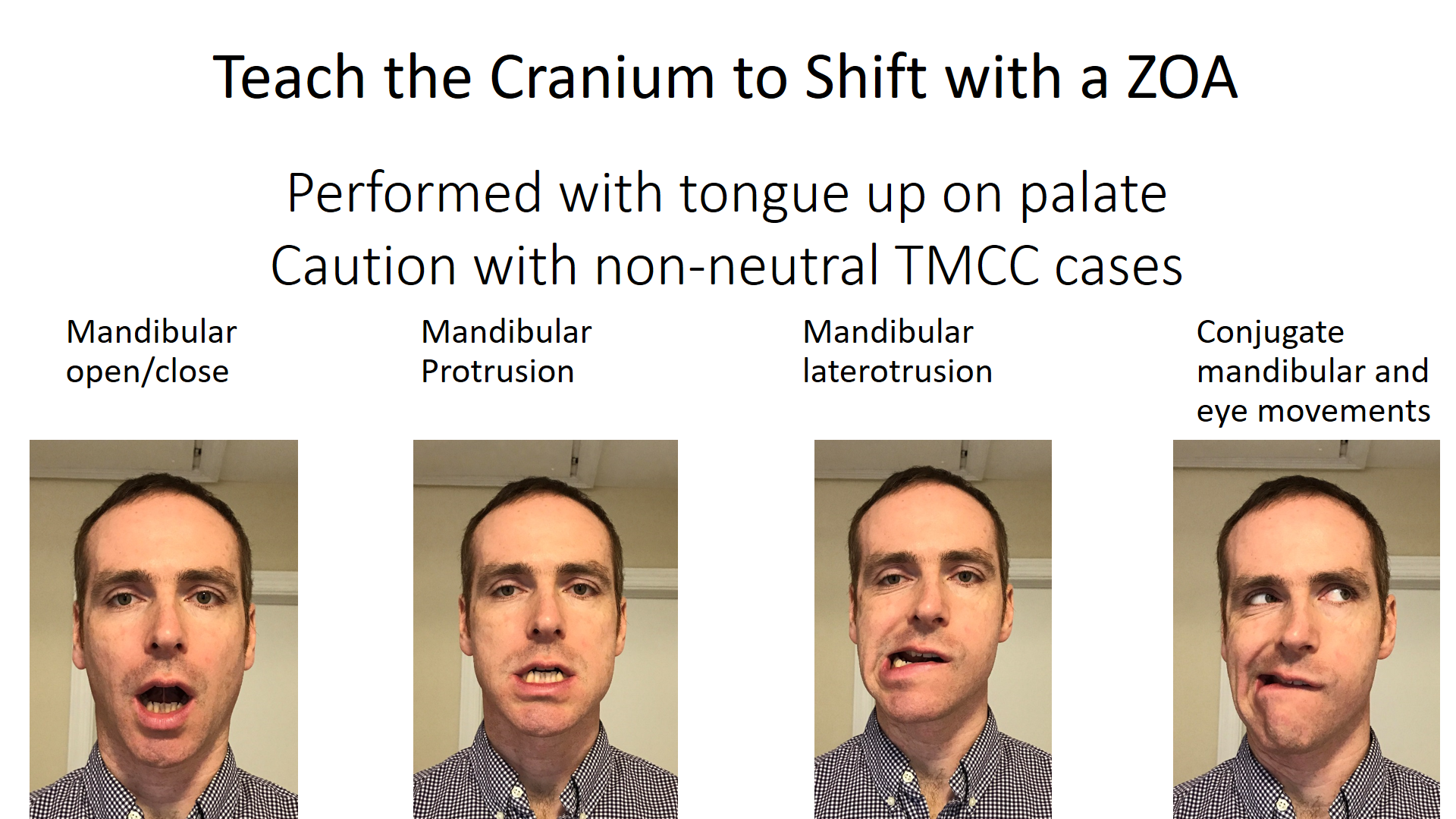
Once one has the ability to achieve a cranial ZOA they need to learn how to shift the rest of their cranium in this new relationship. This involves moving the jaw, face, and eyes in different directions while maintaining a cranial ZOA. This also brings us to another integration point between PRI and OMT. If the TMCC is not neutral please take caution with performing these activities. If you perform them on a non-neutral cranium, more specifically temporal bones that are not neutral, you could potentially be irritating the TMJ and/or other cranial relationships. For example, if one experiences any clicking, popping, or pain in their jaw/face/head they likely are not neutral and thus require specific PRI TMCC intervention before integrating these shifting activities. In the PRI world, this is analogous to establishing neutrality and authentic L and R stance positions at the pelvis and thorax before teaching alternating movements.
Another point to reinforce regarding integrating OMT and PRI is that it will be easier to establish a cranial ZOA when one is neutral. The neuromuscular patterns that facilitate the tongue resting on the palate are paired with neutrality of the AIC, BC, and TMCC patterns. If you question your patient/client about the ease with which they can keep their tongue up when neutral vs not neutral you likely will see this pattern.
Intimately paired with establishing a cranial ZOA is what I refer to as “facial hole control.” For those in the PRI world, “hole control” is typically associated with the pelvis. From a craniofacial perspective, we want our lips sealed so that airflow is only going through the two holes in the nasal cavity vs a hole in the mouth such as with mouth breathing.

Nasal breathing is a big deal for multiple reasons. Nasal breathing warms and humidifies air for improved gas exchange vs mouth breathing which can be very dehydrating. It is via airflow through the nasal cavity which promotes nitric oxide (NO) production. NO is a powerful anti-microbial agent and serves to sanitize the air we breathe. This can also impact the type of microbiome colonies in the oral cavity and gut. NO is a vasodilator which has implications for improving gas exchange in the lungs as well as influencing blood pressure. Finally, there is a significant difference between airflow volume when comparing nasal vs oral breathing. Mouth breathing is characterized by ~12-15 L/Min vs ~6L/min with nasal breathing. This is significant for two reasons. One, increased ventilation volumes promote hyperventilation patterns with decreased CO2 concentrations. This can impact O2 exhange as the presence of CO2 is required for O2 to be released from hemoglobin and utilized by the body. One of the triggers of central sleep apnea can be altered blood gas levels. Therefore, if CO2/O2 levels are shifted due to excessive ventilation the body may stop breathing in order to attempt to increase CO2. Increased airflow volume can also facilitate obstruction in the airway. A higher volume of air moving through the airway will create a higher negative pressure in its wake thus leading to an increased likelihood of collapse. For more information on these concepts I recommend looking into the Buteyko Breathing method (http://www.buteyko.co.uk/).
Before attempting to teach someone how to breathe through their nose, please ensure that they have the ability to do so. An easy test is to see if they can comfortable breathe for 1 minute with their mouth closed. If not, I recently learned a great “nasal clearing method” from Patrick Mckeown, one the premier Buteyko instructors. When one is habitually mouth breathing this can promote “swelling” of the tissues in the nasal cavity as well as tonsils and adenoids. To perform:
1. After a normal exhale pinch off your nose and close your mouth (hold your breath).
2. Keep holding your breath until you feel the urge to breathe in.
3. While doing so move your head forward/backward, side to side, tilt to tilt. This motion helps to flush any excessive fluids out of the nasal cavity.
4. Repeat 4-5 times
5. Determine if helps enable one to breathe through their nasal cavity with lip seal.
If this works then great! You can recommend this technique in conjunction with other techniques that will help promote nasal breathing/lip seal. If there is still congestion, one may need to consider allergies which are common co-morbidities with mouth breathing. Dairy allergies in particular seem to be very mucous producing in the sinus area. To rule this out, I recommend a 3 week elimination of dairy to test whether this is influencing sinus congestion. However, there can be a host of many other possible allergens and thus getting tested for these can be helpful.
If after the above has been considered and there is still an incapability of breathing freely through the nose a referral to an ENT and/or a Dentist with experience in sleep medicine is recommended. ENTs can offer surgical options for increasing space in the nasal cavity. Dentists doing palatal expansion can influence the structural architecture of the nasal cavity (the palate is the floor of the nasal cavity) and create more physical space for air to flow. Palatal expansion can change mandibular/maxillary relationships which can also promote improved airway patency. Finally, palatal expansion can influence the neuromuscular relationships of the orofacial/pharyngeal complex in such a way as to create improved breathing patterns. There are different types of palatal expansion options available such as “Orthotropics”, “DNA Appliance,” and the “ALF.” This process can be implemented on both children and adults with the overall theme, “the younger you start the better.” One of the world’s leading experts in the ALF, Dr. James Bronson, prefers to start this process as soon as the deciduous molar teeth are in which is typically around age 2-3.
Once an affirmative establishment of nasal breathing has occurred it is time to train habitual “hole control.” It is common for chronic mouth breathers to have an over-active mentalis activity (chin muscle that brings the lower lip up) in attempt close their mouth. If this is the case, a great technique I learned from a myofunctional therapy giant, Kathy Winslow, RDH, COM, is to physically pinch the mentalis during the techniques to help inhibit it. Otherwise, a big focus on obtaining lip seal is to facilitate the obicularis oris, particularly the upper fibers. There are many ways to accomplish this goal. Variety can be helpful in keeping the techniques novel and thus more likely to be complied with. It also provides more sensorimotor opportunities to ultimately learn this important pattern.
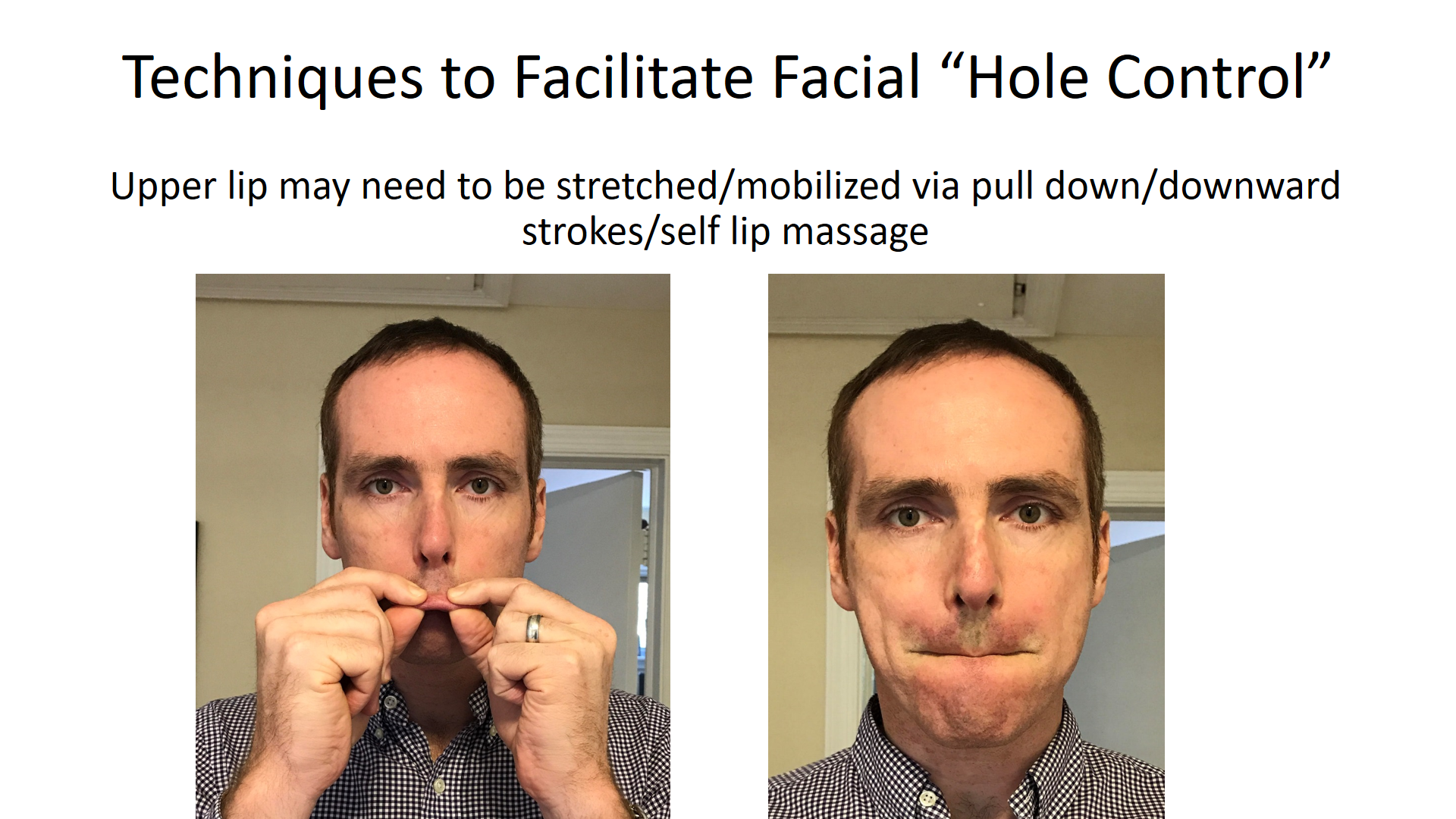
Just like how the tongue may need to be fascially mobilized, the lips may need to be stretched due to fascial restrictions. This can be done by stretching and massaging the lips:
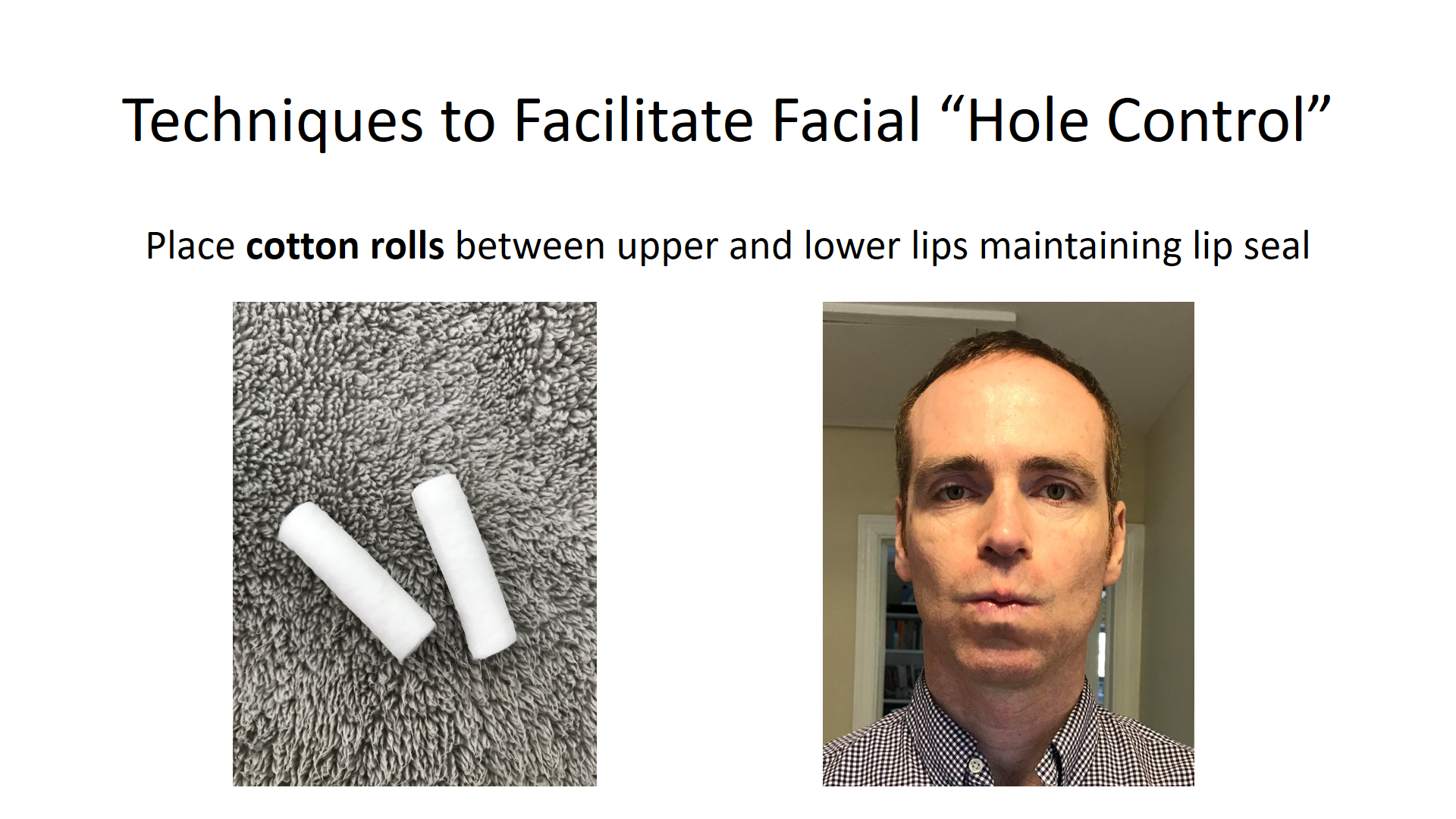
Placing cotton balls inside the upper and lower lips and maintaining lip closure is one option to reinforce this pattern:
Using a tongue depressor, index card, or any other object between the lips is another option for facial teaching habitual “hole control.”

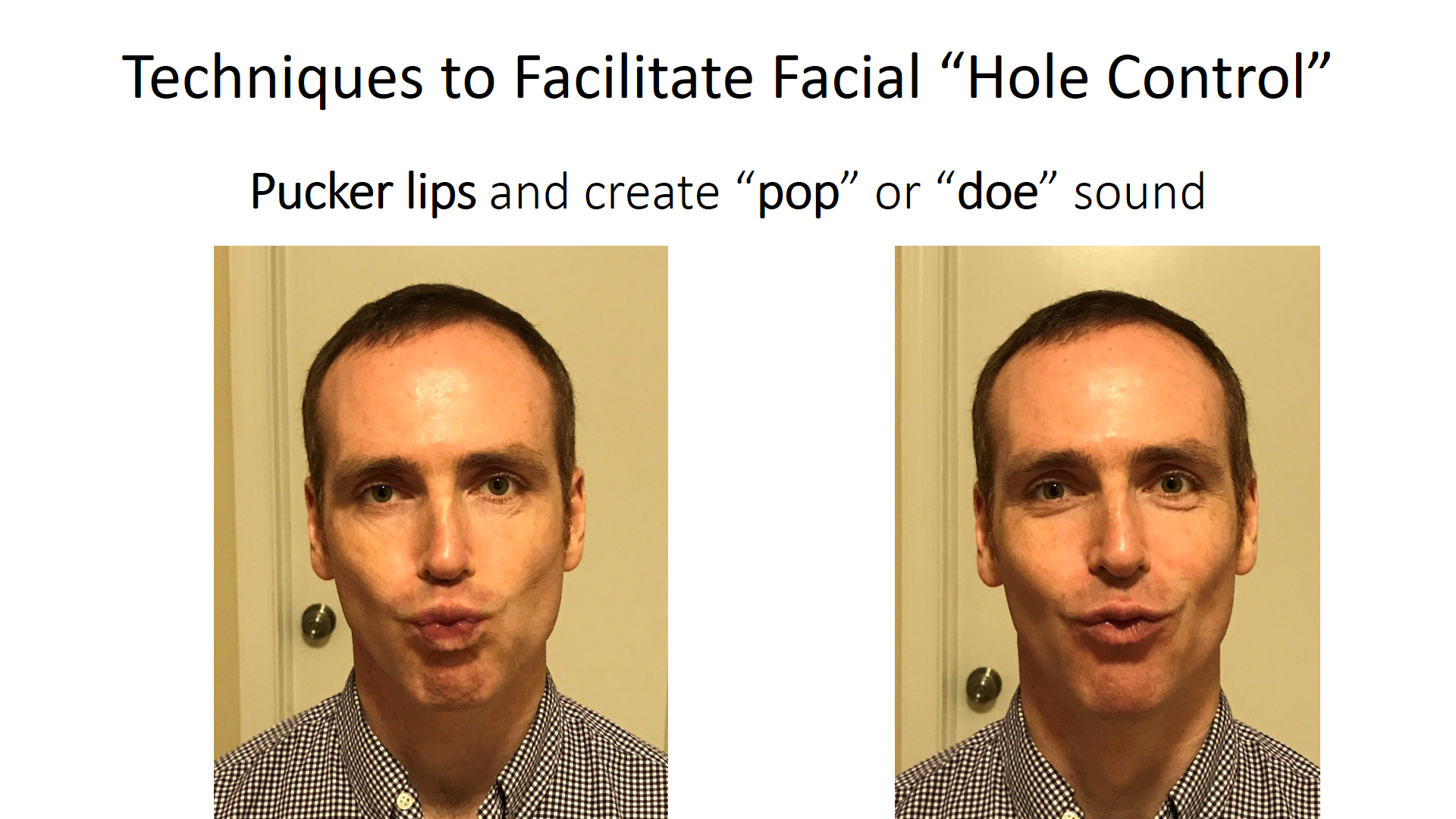
Puckering the lips to create a “pop” or a “doe” sound can be performed:
Using air or water, and maintaining a cranial ZOA, sequentially puff the upper lip, lower lip, and each cheek holding for about 5 seconds each, 5 x each.

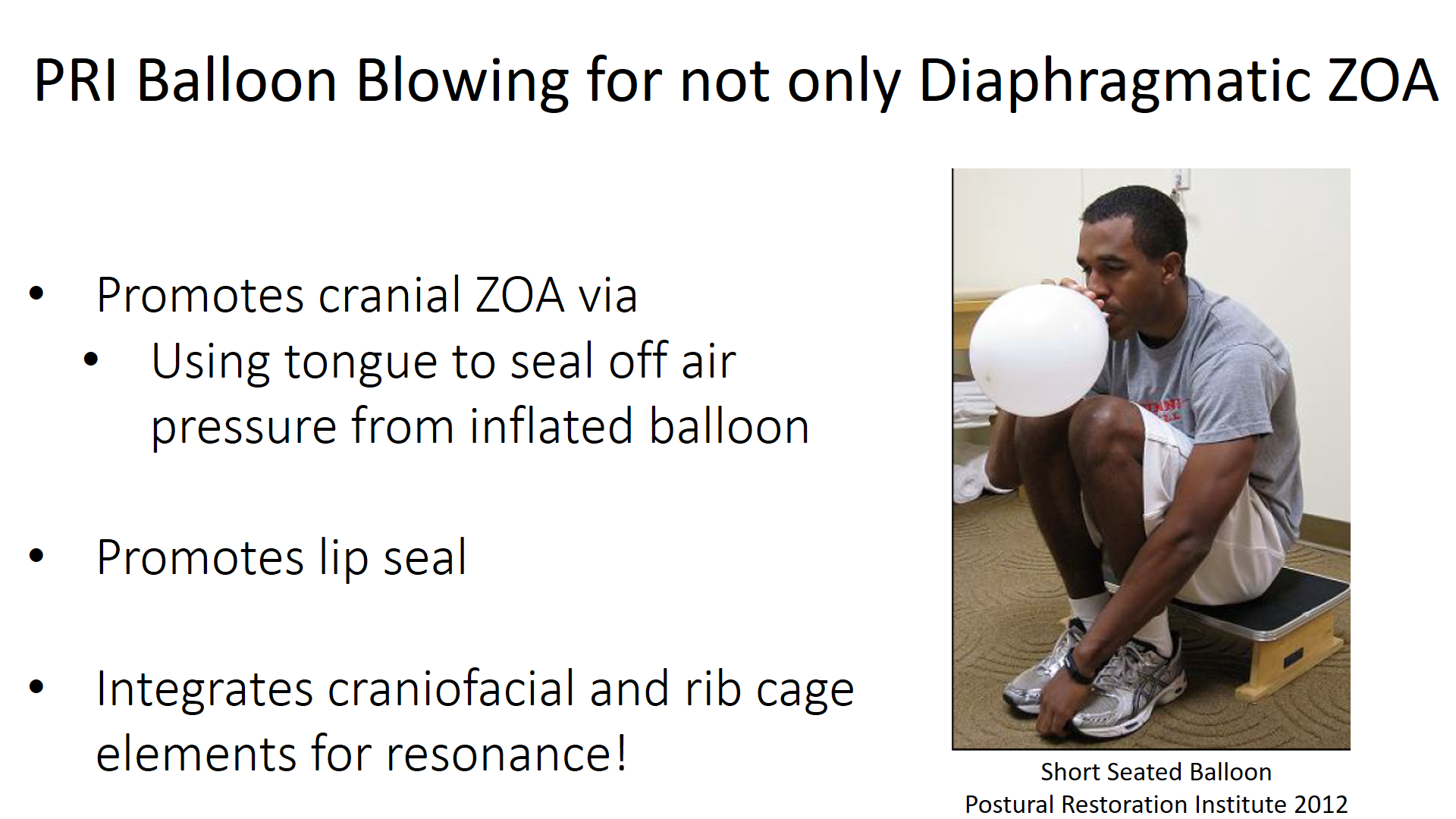
This brings us to another integration point between PRI and OMT, which is balloon blowing. The mainstream PRI perspective of doing progressive balloon blowing with a ~4 sec pause after exhale is to restore the diaphragmatic zone of apposition. This means facilitating the diaphragm (particularly the left leaflet) to become more “domed” and in apposition to the rib cage thus allowing improved inhalation/exhalation function. To see the specifics of the PRI balloon blowing sequencing please refer to this video where Ron Hruska, the originator, is instructing it. What is not typically considered with PRI balloon blowing though is that Ron also designed this technique to impact the orofacial neuromuscular system. PRI balloon blowing also facilitates a cranial ZOA as the tongue attempts to seal off the oral cavity to prevent air from escaping the balloon during the pause and inhalation phases as well as “hole control” due to the need to maintain lip seal around the balloon. In fact, in this study by Guillaraes et al (2009), balloon blowing was one of a group of five orofacial exercises proven to significantly reduce sleep apnea episodes. There was also another study by Puhan et al (2006) that demonstrated how didgeridoo playing had a moderate to large effect on reducing components of obstructive sleep apnea. The authors concluded that the didgeridoo playing was effective in its ability to improve function of the upper airway dilators. However, what the authors did not consider as another possible benefit of didgeridoo playing was the impact it had on influencing diaphragmatic and abdominal position and function.
As mentioned previously, nocturnal mouth breathing and its corresponding excessive ventilatory volume can lend itself to both central and/or obstructive sleep apnea disorders due to the potential for hyperventilation and airway collapse. It can be very difficult for habitual mouth breathers to maintain a lip seal during sleep. For some individuals, their anatomy lends itself to an increased vertical facial dimension creating an extra challenge for lip closure. In these cases, it is highly recommended that these individuals tape their lips together at night. It can take a little time to get used to, but can be very effective in improving sleep quality and accompany subjective sensation of feeling more rested upon waking in the morning.
 We can now move onto the “upward and backward” swallow pattern vs an anterior tongue thrust pattern. A normal swallow pattern involves the tip of the tongue moving up and fulcruming against the palate while the body of the tongue moves posteriorly in a wave-like motion against the roof of the mouth. The facial muscles are relaxed and light occlusal contact occurs. This is opposed to an anterior tongue thrust pattern where the tongue pushes forward and the cheeks suck inward (may see facial grimacing) to create the seal and pressure gradient required for the swallow. Anterior tongue thrusts are typically associated with malocclusion and anterior open bites as demonstrated below (http://www.speechbuddy.com/blog/wp-content/uploads/2012/02/speech10.jpg).
We can now move onto the “upward and backward” swallow pattern vs an anterior tongue thrust pattern. A normal swallow pattern involves the tip of the tongue moving up and fulcruming against the palate while the body of the tongue moves posteriorly in a wave-like motion against the roof of the mouth. The facial muscles are relaxed and light occlusal contact occurs. This is opposed to an anterior tongue thrust pattern where the tongue pushes forward and the cheeks suck inward (may see facial grimacing) to create the seal and pressure gradient required for the swallow. Anterior tongue thrusts are typically associated with malocclusion and anterior open bites as demonstrated below (http://www.speechbuddy.com/blog/wp-content/uploads/2012/02/speech10.jpg).

If an individual has a cranial ZOA and lip seal issues it is likely that they also are not swallowing properly as these three patterns tend to co-occur. However, before training correct swallowing, one must be able to have an authentic cranial ZOA. Once that has been established, techniques may be considered to help reinforce an “up and back” swallow pattern. Initially, swallow training is characterized by keeping the lips apart. This is to help reduce the facial grimacing. There is also a gentle “bite” component with the techniques. This topic is beyond what is to be covered in this article but it is worth mentioning the importance of proper occlusion with regards to swallow patterns. There may be some individuals who avoid the bite due to malocclusion while there may be other situations where the maloccluded bite can be creating undesirable temporal cranial cervical mandibular neuromuscular relationships. In the PRI world, this is typically associated with the TMCC patterning. Therefore, it may be necessary to have the bite addressed through dental integration.
The first technique to be discussed is the “K” Swallow. Practice saying “K” or “Kaw” ~5 times (facilitates posterior tongue/palate contact), gently bite, keep lips open, and swallow. Next there is the “Water Trap Swallow” where one takes a small sip of water, traps it up against the palate (may need to tilt the head), gently bite, keep lips open, and swallow. Another technique is the “Pencil or Chopstick Swallow” where one gently bites down on either a pencil or chopstick which makes it difficult for the tongue to posture anywhere but up during the swallow.
After the mastery of these swallow techniques, one must begin to functionally integrate the “up and back” swallow pattern during meals. Just like how achieving a habitual cranial ZOA initially requires significant cognitive effort, implementing a new swallow pattern can as well. Therefore, eating and drinking takes on a certain type of mindfulness as one is attempting to reinforce the new habit. Since we have reached the topic of eating it is also worth pointing out the importance of being able to alternate chewing on each side. This is another integration point with PRI. With the typical R TMCC pattern, an individual is more inclined to chew on their right side vs their left. Chewing is analogous walking as it represents an alternating lateralized behavior or we may refer to as “resonance.”
Finally, as one establishes mastery of their cranial ZOA, facial hole control, and up and back swallow, integration with the rest of the postural system may be warranted to be able to achieve not only craniofacial but entire body resonance. Therefore, depending on the specific needs of the individual, any OMT technique may in combined with any PRI technique. Below are some examples where lip seal techniques are being integrated with upright reciprocal PRI techniques. There are so many potential ways to integrate. Be creative and channel your inner Heptapod!
